ZYGOMATIC ARCHES
Tangential Projection • Submentovertex • Zygomatic Arches and Cheekbones Evaluation

Exposure Factors
Moderate exposure: Intermediate between skull (70-75 kV) and nasal (50 kV)
Plate Size and Orientation
Transverse orientation to include both zygomatic arches
Optimal Image Characteristics
- Bilateral symmetrical SMV images of both zygomatic arches
- No overlapping structures obscuring the arches
- Symmetrical zygomatic arches (right vs left)
- Head without rotation - Mid-sagittal plane perfectly perpendicular
- Arches clearly projected, without overlap with parietal eminences
Common Technical Challenges
Zygomatic arches may project behind parietal eminences when:
- Arches are anatomically very flat
- They are depressed by trauma
- They are far from IR (image receptor)
- The divergent beam projects them incorrectly
Solution: Adjust angulation and verify that IOML is parallel to IR
Zygomatic Arches Anatomy
Zygomatic Arch
Cheekbone bony structure
Temporozygomatic Junction
Articulation with temporal bone
Maxillozygomatic Junction
Articulation with maxilla
Frontozygomatic Junction
Articulation with frontal bone
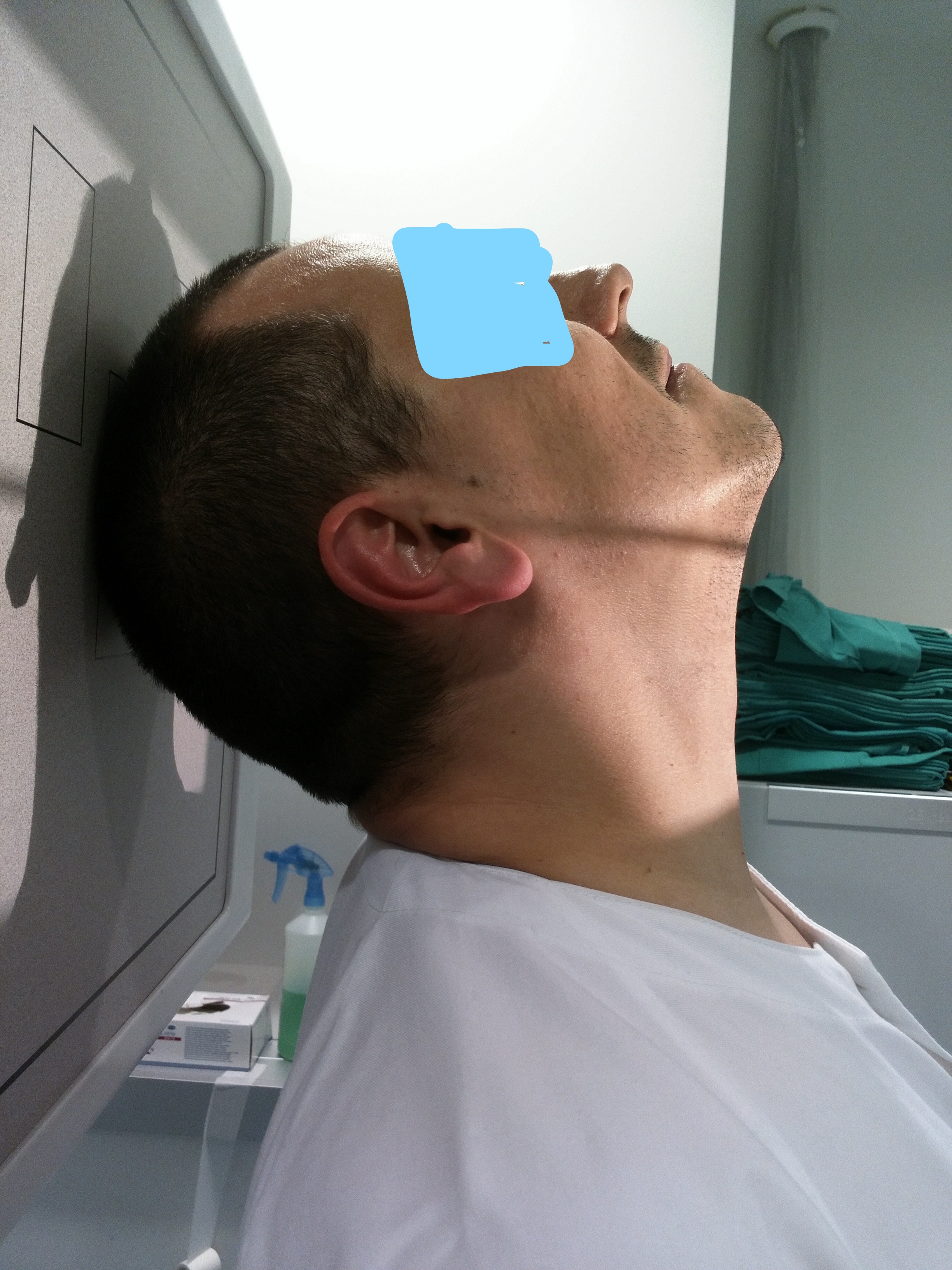
COMPLETE NECK HYPEREXTENSION
This projection requires maximum neck hyperextension to achieve:
- IOML parallel to IR plane
- True tangential projection of arches
- Avoid overlap with other structures
Alternative: Use vertical cephalic unit when patient cannot hyperextend
Patient Positioning
Exact Central Ray Point
Location: Mid-sagittal plane of throat
Reference: From external eye canthus backward
Trajectory: Perpendicular to IOML
Direction: From bottom to top (submentovertex)
Central Ray Direction
PERPENDICULAR to IOML
Entry point: Mid-sagittal plane of throat
Exit point: Vertex (crown)
Trajectory: Submentovertex (SMV)
Image Receptor Centering
"IR is centered on the central ray"
The image receptor (IR) must be perfectly centered with the central ray to:
- Capture both zygomatic arches symmetrically
- Avoid cutting anatomical structures
- Maximize useful field of view
- Minimize patient dose
Patient Instructions
"Hold your breath during exposure"
Maintain complete neck hyperextension without moving during exposure
Zygomatic Trauma Considerations
Movement Limitation
In severe trauma, patient may not be able to hyperextend completely.
Alternative Position
Use vertical cephalic unit or modify angulation according to tolerance.
Complete Fractures
Look for discontinuity, displaced fragments, asymmetry.